Why is the Rh D- type important in pregnancy?
Babies inherit their blood type from both biological parents. This is important because if you are pregnant and have a D-negative blood group, it is possible the baby you carry will have D-positive blood group, having inherited this from the other biological parent.
However, it is important to know; it is possible even when one parent is Rh-D positive and one parent is Rh-D Negative, the baby may still be Rh-D negative based on how the blood group is inherited.
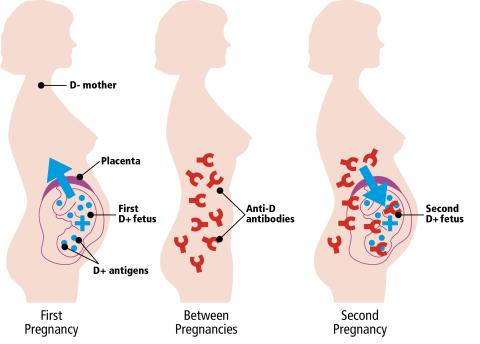
Inside the womb, the placenta usually acts as a barrier between maternal red blood cells and the baby’s. However, even in normal pregnancies small amounts of the baby’s blood may cross over into your blood stream. The most common time for a baby’s blood cells to get into your blood is when you give birth.
If any of the blood cells from an Rh-D positive baby get into the Rh–D Negative maternal blood stream, your body recognises the D antigen on your baby’s blood cells as a foreign protein and may produce antibodies to it.
This is called ‘sensitisation’. Any event or circumstance that could cause the pregnant patient to produce antibodies against the D antigen is called a ‘potentially sensitising event’ (PSE).
Examples of PSE include a miscarriage or termination of pregnancy, or if something happens during your pregnancy such as having an amniocentesis (a test to check if your baby has a genetic or chromosomal condition), chorionic villus sampling (genetic testing), vaginal bleeding or after abdominal injury such as a fall, a blow to your abdomen or trauma from a seat belt.
As a general rule, the first pregnancy that triggers this sensitisation, does not cause the baby suffer any adverse consequences, as it will already have been born by the time antibodies have developed.
However, if you become pregnant again with a D-positive baby, there is a possibility, the anti-D antibodies may cross into the baby’s bloodstream and attack the baby’s red blood cells.
This is called ‘haemolytic disease of the fetus and newborn’ or ‘HDFN’.
HDFN can be mild, but if more severe can lead to anaemia, heart failure, jaundice, brain damage, or even to the death of the baby.
With further pregnancies and further D-positive babies the risk of earlier and more severe HDFN increases and the outcomes can be more serious. This is why a preventative measure such as the use of anti-D prophylaxis is so important.
There are about 65,000 births of D-positive babies to D-negative pregnant people in England and Wales each year. It is estimated that, without routine preventative treatment, there would be over 500 problem pregnancies each year, leading to the deaths of over 30 babies and more than 20 brain damaged children.
With acknowledgement to NHSBT Patient Blood Management Practitioner Team, and CSL Behring UK Ltd for kind permission to use text from their anti-D leaflet.
Protecting you and your baby with anti-D immunoglobulin - patient information leaflet
Review due: April 2026